Content warning: This article discusses delays in medical care, denied insurance claims, corporate abuse, and financial stress on patients.
“Approved Before Surgery. Denied After Surgery.”
In a short, quietly devastating clip, an American surgeon explains a pattern that sounds like a bad joke — except it’s how one of the biggest health insurers in the world actually does business.
He describes how a major insurer requires prior authorization for many surgeries. The doctor’s office sends all the clinical details, the insurer reviews everything and approves the surgery. The patient goes under the knife believing they are covered.
Then, after the surgery is done, something else happens:
AdvertisementAround 40–50% of those same, pre?approved procedures are denied when the hospital submits the bill.
Nothing new has changed medically. The only new document is the procedure note — the description of the surgery that was just performed. The underlying clinical information is exactly the same as what the insurer already reviewed when it granted prior authorization.
So what is really happening?
The doctor spells it out: this is delay, not new evaluation. The claim is bounced back, the office is told to re?submit medical records for “clinical review,” the clock is restarted, and the insurer buys itself time and friction — hoping, in many cases, that the claim will be reduced, written off, or quietly abandoned.
For patients and clinics, it feels less like “health insurance” and more like a financial obstacle course laid over the top of medicine.
Recommended Product
Jockey Women's Hipster Brief – Comfort Fit, Assorted Colors
🛒 View on Amazon →As an Amazon Associate, we earn from qualifying purchases. Price and availability may vary.
Real People Behind The Numbers: Denied, Dragged Out, And Left With Bills
The comments around this clip read like case files from a system that’s forgotten what its product is supposed to be.
“I did everything right and still paid ?3 lakh–plus equivalent”
One person describes turning 45, the new recommended age for a first colonoscopy. They weren’t just ticking a box — they had:
- active bleeding,
- chronic digestive issues, and
- a strong family history of colon cancer.
On paper, they met multiple “medical necessity” criteria. Yet the procedure was denied as “not necessary.” They paid the entire amount out of pocket — over the equivalent of ?3.3 lakh — despite clear risk factors. The colonoscopy revealed multiple polyps, which were removed, vindicating the decision to proceed.
They appealed twice as the insurer slowly dragged the process out. The answer never changed. No coverage. No remorse. Just a lesson: even when you match the rulebook, the system can still shrug and walk away.
“They ran down the clock by restarting the review”
Another person talks about getting prior approval, going through with care, and then being told that a fresh form had not been filled — a trivial attestation that this was their only insurance. By resetting that one checkbox, the insurer restarted a 30?day review clock. The outcome is still pending, but the pattern is familiar: drag things out long enough and some patients will give up or settle for less.
Watching these stories pile up, a common reaction emerges: this mess looks ripe for a class?action lawsuit.
“They told me to do conservative treatment for six years, then denied the tests they demanded”
One commenter describes a large insurer insisting they cancel a scheduled, necessary surgery and instead go through more “conservative management” — physiotherapy, drugs, steroid injections. The problem? They had already done exactly these treatments for more than six years.
The story gets worse:
- The insurer then pre?authorised an MRI and X?ray that doctors required before proceeding with injections.
- The hospital did the imaging.
- Months later, the insurer told the hospital that the policy was “out of network” and refused to pay about $3,000 in bills — despite having approved the tests up front.
- The hospital, in turn, threatened to send the patient to collections.
In short: “Do PT and injections first, then we’ll consider surgery.”
Patient does PT and injections.
Insurer then refuses to pay for the very scans they demanded, citing a network technicality at a hospital that had been in?network for a decade.
“I even got a bill from an insurer I never had”
Someone else describes going to urgent care, having their existing insurance pay the visit, and then receiving a separate bill from another giant insurer they were never enrolled with — charging them over $1,400 in premiums. From their perspective, this looks less like a clerical error and more like fraud wrapped in bureaucracy.
Not Just One Company, Not Just One Industry
The doctor in the video names one insurer. The replies describe others behaving similarly. Patterns repeat:
- Approve in advance, deny after the fact.
- Demand extra paperwork after the surgery, based on criteria that existed before.
- Declare “network changes” months after care is given.
- Use small technicalities to restart review clocks and delay payment.
One person draws a line back to consulting playbooks used in other industries, including tactics installed at large property insurers:
- Make the claims process as exhausting and opaque as possible.
- “Improve efficiency” by training staff to wear down claimants until some walk away.
- Frame it as operational excellence while quietly shrinking payouts and boosting profits.
In that model, the core business quietly shifts from “taking premiums and paying valid claims” to collecting premiums and carefully not paying whatever can be avoided.
The Public Is Funding The Game
A particularly sharp observation in the discussion points out that taxpayers are underwriting a large part of this behaviour.
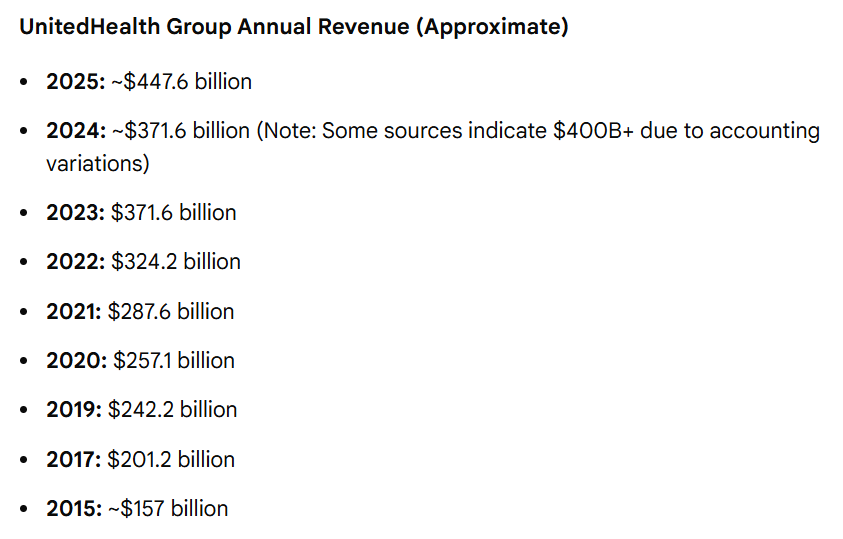
- The insurer named in the doctor’s clip now gets more than three?quarters of its revenue from government programs — Medicare Advantage, Medicaid plans and other taxpayer?backed contracts.
- A big chunk of that growth has come from seniors and low?income people enrolled in these plans, often because they have no better option.

So when half of certain authorised surgeries end up denied after the fact, it is not just private employer plans that are affected. It hits:
- older adults on Medicare?type products,
- low?income families on Medicaid, and
- the public budgets that fund those programs.
One commenter summarises it bluntly: “It seems to be working — and we’re the ones paying for it.”
Why This Keeps Happening: Incentives And Loopholes
To be fair, insurers defend prior authorization as a tool to prevent unnecessary procedures, control costs, and ensure care is appropriate. There is truth in that. Prior auth can stop genuinely inappropriate or duplicative care.
But several trends have made it a blunt instrument:
- Prior authorization has expanded from a narrow set of high?risk or high?cost procedures to a wide range of routine treatments, increasing friction on everyday care.
- Investigations into major plans, including Medicare Advantage carriers, have found that prior auth and denials are sometimes used in ways that systematically squeeze expensive care, especially post?acute or complex services.
- Providers and medical associations argue that the process now often serves to delay and discourage care, and to delay and discourage payment, rather than simply vetting clinical appropriateness.
From patients’ vantage point, the design looks obvious:
- If you deny or delay a large enough slice of claims, some percentage of people will never fight back.
- If you restart the clock often enough, some clinics will write off smaller amounts as uncollectable.
- If you make appeals time?consuming and confusing, you keep more money — even if the underlying care was justified.
That’s why some voices are now calling for basic structural guardrails.
One concrete proposal being floated is a federal rule that every denial must be signed by a licensed physician, clearly state the clinical rationale, and include that physician’s name, national provider identifier and licence details. The idea is simple: if a human being with a licence has to put their name on each denial and reasoning, the casual, anonymous “rubber?stamp” denials become harder to hide and easier to challenge.
What Patients Can Do In A System That Feels Rigged
None of this is easy to fix at an individual level, but there are some practical moves that can reduce your odds of being steam?rolled.
Before surgery or major procedures
- Ask for everything in writing. Get written confirmation of prior authorization, including procedure codes and any network confirmations. Keep copies of all letters, emails and approval numbers.
- Double?check “network” status yourself. Don’t rely solely on verbal assurances; confirm via the insurer’s website or written communication that the hospital and doctor are in network, especially if your plan has changed recently.
- Clarify what could trigger a later denial. Ask the clinic’s billing office if they’ve had similar procedures denied after prior auth and why. Learn whether certain add?on codes or complications are frequently questioned.
If you get denied after prior approval
- Appeal, and appeal in writing. Refer specifically to the prior authorization approval and include a timeline. Ask the insurer to explain, in clear language, what new information justifies reversing their own earlier decision.
- Use every escalation path. Request an internal appeal, then an external review where available. In publicly funded programs, contact relevant ombudsman or regulator offices.
- Coordinate with your doctor’s office. Many clinics have staff who deal with this daily; they can help frame the medical necessity arguments clearly and provide the exact documentation insurers expect.
- Document patterns. If you see a recurring type of denial or clock?reset trick, keep records. These are the raw material for complaints to regulators, journalists, or, eventually, lawyers building systemic cases.
At the policy level
Individually, people can only push so far. Systemically, this moment is part of a larger backlash:
- Regulators and legislatures are scrutinising prior auth delays and denials, especially in government?funded plans.
- Large medical associations are now openly calling for transparency around how much insurers profit from unnecessary prior authorization hurdles.
- Under public pressure, some big insurers have pledged to reduce prior auth volumes and speed up decisions — but providers argue that, on the ground, little has changed yet.
The fact that a practising surgeon now feels the need to go on camera and say “half of our supposedly approved cases are denied afterward” should be a red flag, not just a viral soundbite.
The Real Question: What Business Are Insurers In?
At the end of the clip, the doctor confirms the core truth: the clinical information under review before and after surgery is basically the same. The difference is timing and leverage.
Before surgery, the insurer holds power by threatening to block care.
After surgery, it holds power by threatening to stick the patient or hospital with the bill.
If the same facts can lead to “approved” when a patient is unconscious on a table and “denied” when the invoice arrives, then we are no longer talking about medicine or even risk management. We are talking about a financial system that has learned to profit from exhaustion, confusion, and delay.
The people in that comment thread — with their unpaid colonoscopies, cancelled surgeries, phantom bills and endless appeals — are not edge cases. They are the logical outcome of a machine that forgot its product is supposed to be care, not denial rationales.
And until the cost of this behaviour is higher than the savings it creates, no viral video — no matter how clear — will be enough to make it stop.
